By Diena Seeger, iBalans LLC
Senior populations commonly experience falls, and poor balance is one of the major risk factors. Research suggests that improvements in dynamic balance can assist in the reduction of falls. iBalans, the company that created the WAV, conducted a small-scale test of a robust approach to balance training and assessment within a senior population.
Prior to conducting this test, a pilot research study conducted at Jefferson University found subjects (ages 18-40) that engaged in a 6-week exercise program with the WAV Sensorimotor Trainer showed statistically significant improvement in dynamic postural control compared to those who did not use the WAV, based on Y-balance measurements (Doriston, MG, El-Kerdi, AI (2019). Effects of Core Stability Training Using the WAV Trainer to Improve Static and Dynamic Postural Control. submitted for publication).
In light of these measured balance improvements in a relatively young population, the feasibility of implementing WAV sensorimotor training in a senior population and measuring the impact on static and dynamic balance was explored. Consideration was given to the plausibility of the tested methodology in a therapeutic setting to:
- Objectively quantify balance capability,
- Identify fall risk,
- Develop personalized therapeutic plans to address identified concerns, such as postural malalignment, mobility restrictions, impaired coordination, neurological deficits and fear of falling, and
- Determine the effectiveness of WAV training for improving balance via pre and post protocol measures.
For this small-scale investigation iBalans partnered with ProtoKinetics, a leading developer of gait analysis and balance assessment systems, and Body in Balance Physical Therapy and Fitness Center, specialists in the aging population and host of the Parkinson’s Life Center of Southern NJ.
Attention was given to ensure testing equipment and methodology were robust and effective yet safe for people with fall risk. ProtoKinetics chose their Zeno Walkway for collecting data because it is essentially as easy and safe to maneuver as walking on a flat surface. Static and dynamic balance were assessed via Quiet Standing (QS), Limits of Stability (LoS) testing and the Four Square Step Test (FSST), all performed on the 4’x4’ Zeno Walkway (refer to Appendix A: Methodology). Testing was led by Michael Rowling from ProtoKinetics.
Due to the limited scope of this investigation, participants were tested with their eyes open. Older adults, however, are likely to have an increased reliance on visual input for postural control, particularly those at risk for multiple falls. As such, it is recommended to include additional testing with eyes closed when feasible. This would provide a more robust assessment that includes visual sensory information.
Six participants between the ages of 61-80 were broken into two groups with Group 1 considered low fall risk and Group 2 higher fall risk. Participants completed a single 15-minute WAV exercise session appropriate for their group classification led by Dr. Andrea Olsen PT, DPT from Body in Balance (refer to Appendix A for demographics and methodology).
Indication of Sequencing Skills and Dynamic Balance

The FSST is a common assessment used in clinical settings. The FSST duration, in particular, has been validated as an important measure of fall risk. Published research indicates that individuals that experience multiple falls have an average FSST duration of 32.6 seconds (SD 10.1) while individuals that do not experience multiple falls have an average of 17.6 seconds (SD 8.3) (Dite et al. 2007). Moreover, adults who are considered not to be a fall risk can often complete the task in under 10 seconds.
While not yet published, additional FSST measures can be used to provide further insight into fall risk. Generally, adults predicted to be non-fall risk score a 0 for the measure of “over double supports”. Any occurrence of over double supports (i.e. > 0) could imply a balance deficit or at least warrant further investigation. Additionally, the measure of “changes in main support” is typically within 10-20 for non-fall risk adults, with optimal performance scored at 10.
FSST Performance Results
A review of the FSST data (refer to Table 1) indicates that person 5 poses a fall risk and would benefit from balance training to help prevent further decline and potentially reduce fall risk. His baseline assessment shows FSST time in the range of a potential faller, multiple over double supports and changes in main support outside the typical range for non-fall risk adults.
All FSST measures taken post WAV exercise session show notable improvement, including 13% improvement in duration, a full point reduction in over double supports and 17% improvement in changes in main support. These are good indicators that this person would benefit from a WAV training program with exercises geared towards those with higher fall risk like the exercises completed by Group 2.
Persons 1 and 4 performed at a very high level at baseline, without significant gains to be made, so there was not much room for measured improvement. Both baseline assessments show FSST time in the range of an unaffected, non-faller, no over double supports and almost perfect changes in main support (nearly 10).
Further testing is required to determine if persons 1 and 4 did not have balance deficits or the tasks simply were not difficult enough to uncover them. A more thorough baseline assessment including testing with eyes closed and complete dual tasking FSST would be appropriate in this situation. These participants would likely benefit from WAV training with more complex movement patterns and increased focus on sensory integration than the exercises completed by Group 1.
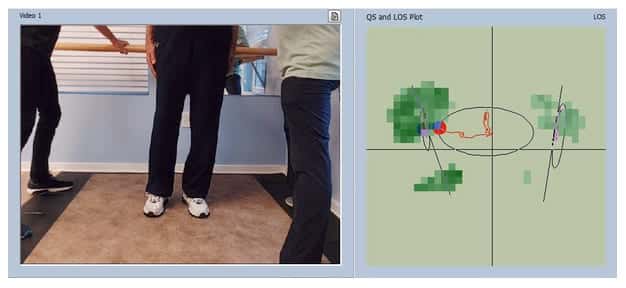
The difference in step pattern during the FSST of participant 5, with potential fall risk, versus participant 1, without fall risk, is easily visible in the output from the PKMAS as shown in Figure 1.

Persons 2 and 3 performed fairly well at baseline. However, the occurrence of over double supports and changes in main support trending towards the upper limits for non-fall risk individuals indicates these participants may benefit from balance training to prevent decline and reduce fall risk. Measures taken after the WAV exercise session showed some improvements, particularly bringing over double supports to 0 for both participants. Like persons 1 and 4, more baseline data would be beneficial for quantifying fall risk and developing training programs that include WAV exercises appropriate for these participants.

Indication of Static Balance and Dynamic Postural Control
Voluntarily changing one’s center of gravity position with control is considered fundamental to independence and the ability to safely complete activities of daily living (ADLs), such as reaching for objects and standing up from a chair. Current literature indicates that balance and sway measurements from bipedal quiet standing are strong predictors of fall risk, however there is no clear consensus as to which single metric or subset is most appropriate to classify “fallers” and “non-fallers.” A common aim of therapeutic interventions is to positively impact fall risk by increasing medio-lateral (ML) and anterior-posterior (AP) mobility along with overall sway.
QS Performance Results
Looking at the relative difference in pre and post measures, some changes in ML and/or AP measures during quiet standing were noted across the participants.
Figure 2 illustrates a 44% improvement in ML mean for person 1 as captured by the Zeno Walkway. This participant started with a baseline of -2.7 cm and showed some improvement with less leftward lean of -1.5 cm post WAV exercises. A minimal change was noted for mean AP measures. Person 4 also showed some improvement in ML mean going from -1.3 cm at baseline to -0.6 cm post WAV exercise.

Participants 3 and 5 had the most forward lean in quiet standing based on AP mean baseline values. Each person showed roughly 20% improvement to stand with less forward lean, moving from a baseline of 3.4 cm to post exercise values of 2.6 cm and 2.7 cm, respectively. Participant 2 saw relatively no change for both AP mean and ML mean values between baseline and post WAV exercise.
LOS Performance Results
WAV exercises had a positive impact on dynamic balance for most participants based on the measured sway (ellipse) area during LoS testing. Figure 3 illustrates a 58% improvement in global mobility for participant 2 as captured by the Zeno Walkway. He started with a baseline average sway area of 165.7 cm and experienced both ML and AP gains that resulted in a 261 cm average sway area post WAV exercises.
Participants 3 and 4 showed roughly 28% improvement in sway area, while person 5 showed 8%. Person 1 showed a 16% decline post WAV exercise which may have been due to fatigue.

Results Summary
Poor balance is one of the major risk factors for falls within senior populations, and research suggests improving dynamic balance can help reduce falls. Safe assessment methods that objectively quantify balance capability and identify fall risk coupled with training approaches that positively impact postural control and engage seniors can be a powerful way to improve dynamic balance and hence reduce fall risk.
Based on the small sample of participants in this investigation, WAV training together with assessment via the Zeno Walkway can be quite positive for seniors. Objective data collected after a single 15-minute WAV training session demonstrated that a balance training program that includes the WAV may positively impact balance metrics important for reducing fall risk for seniors. Additionally, participant feedback indicated that WAV training creates a positive exercise experience that leaves seniors feeling encouraged about their ability to improve their balance.
Observations and participant verbal comments on the ease of testing illustrated that the Zeno Walkway can be a safe and effective solution for quantifying balance capability, even in senior populations that may have fall risk or impaired physical mobility.
For seniors that exhibit good balance control, such as some of the participants in this investigation, it is recommended to perform additional baseline assessments that account for visual sensory information and multi-tasking. This would provide more robust data for developing personalized WAV sensorimotor training programs and better quantify pre and post training fall risk in such cases. While not completed in this test due to time constraints, the additional data can be collected using the same equipment and approach outlined.
Appendix A
Demographic and Biometric Data
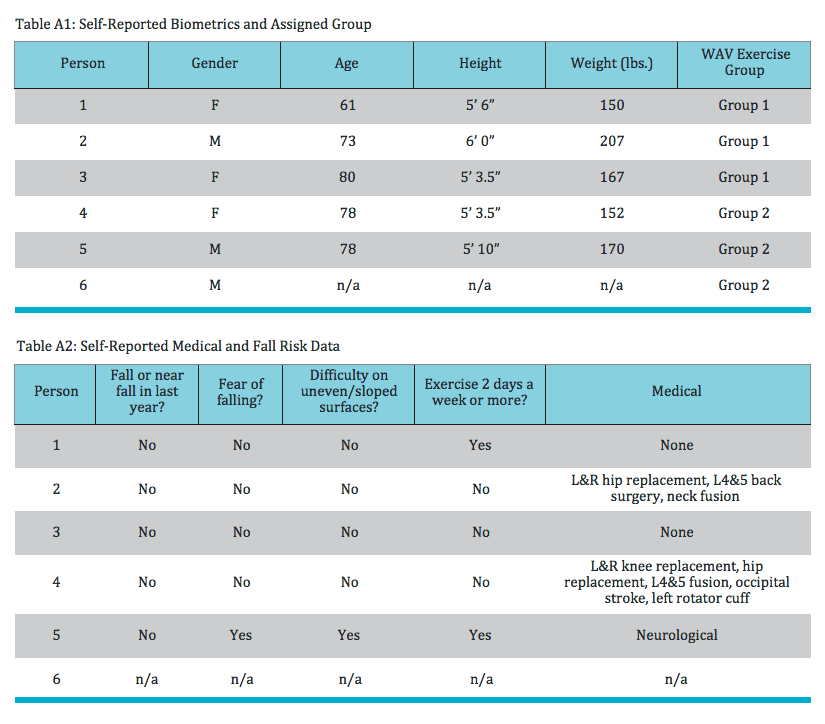
Six participants between the ages of 61-80 were recruited at random and did not receive compensation for their participation. Table A1 presents participant self-reported demographic and biometric data. It also includes the assigned exercise Group as determined by Dr. Andrea Olsen based on self-reported data and a short verbal interview. Table A2 presents participant self-reported medical and fall risk data collected at baseline. Participant 6 only participated in the group exercise session and chose not to participate in written data collection or objective testing.

Methodology
After completing self-reported medical and fall risk data forms, all participants were asked to participate in baseline testing for QS, LoS and FSST prior to their exercise session. These pre-exercise measures were taken as follows:
- Participants watched a demonstration of QS and the LoS test given by Dr. Olsen
- Participants completed 1 practice run of QS and the LoS test
- Participants completed 2 scored trials of QS and LoS testing
- Participants watched a demonstration of the FSST given by Dr.Olsen
- Participants completed 1 practice run of the FSST
- Participants completed 2 scored trials of the FSST
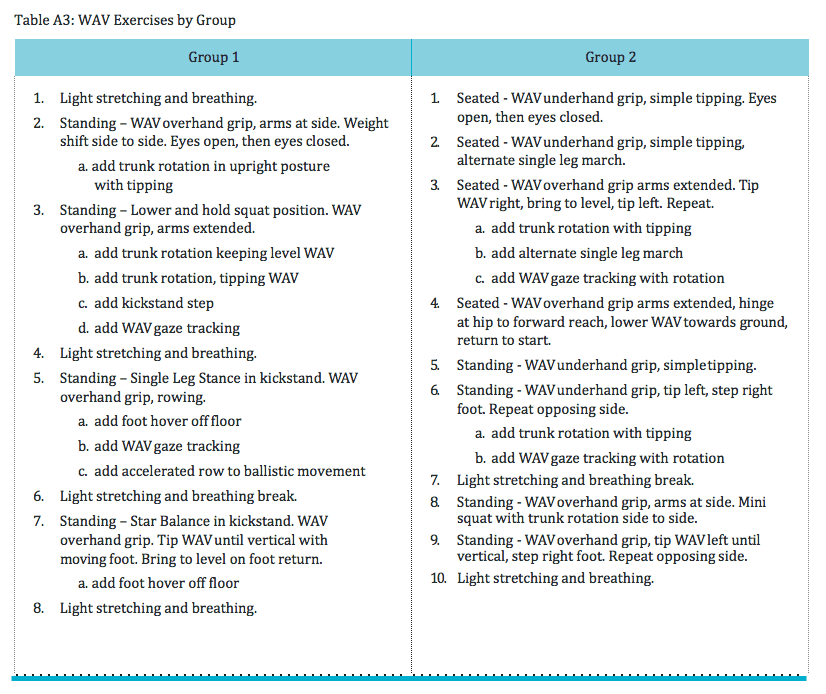
Under the direction of Dr.Olsen, Group 1 was led through WAV exercises appropriate for lower fall risk individuals and Group 2 was led through WAV exercise appropriate for higher fall risk individuals. Group 1 performed WAV exercises with dynamic movement patterns in standing position. Group 2 performed WAV exercises both seated in a chair and in modified standing positions. Exercises chosen were based on the WAV foundational training principles, the Sensory 7, and modified as appropriate for the fall risk classification of the group (refer to Table A3).
Dr. Olsen educated each group on the exercises, gave demonstrations and then led each group independently through a 15-minute training session, providing guarding, hands on direction and verbal instruction as appropriate. Due to the very limited nature of this investigation, no personalization or modifications to exercises were provided. All participants within a group were instructed to complete the same set of exercises.
Following their exercise session, participants from each group completed 2 scored trials of QS, LoS testing and the FSST. The temporal, spatial and pressure measurements collected were analyzed with ProtoKinetics Movement Analysis Software (PKMAS). Participants were also asked to complete a questionnaire about their experience. Person 6 only participated in the group exercise session and chose not to participate in written data collection or objective testing.

Quiet Standing (QS)
QS was measured by having the participant remain in a standing position on the Zeno Walkway with a fixed gaze for 20 seconds to measure displacements of the center of pressure (CoP) of each foot. The PKMAS software provided 20 data points that gave insight on stability and postural control during standing including sway area, path length, and anterior- posterior (AP) and medio-lateral (ML) movement.

Limits of Stability (LoS)
LoS are defined as the points at which the center of gravity (CoG) approaches the limits of the base of support (BoS) and a correction strategy is essential in order to return the center of mass (CoM) to within the BoS. Simply put, an individual’s LoS is the maximum excursion they are able to intentionally cover in any direction without experiencing loss of balance or taking a step.
LoS was measured immediately after the participant completed QS (without moving their feet or foot position). Remaining on the Zeno Walkway, participants reached their maximal position in four directions (forward, right, backward and left) coming to a quiet stand position between each direction. The PKMAS software provided 18 data points that gave insight on voluntary motor control in the dynamic state including sway area and anterior-posterior (AP) and medio-lateral (ML) mobility.
Four Square Step Test (FSST)
The FSST is a dynamic balance test assessing a person’s ability to step over objects in the forwards, sideways and backwards directions. PVC piping was placed on the Zeno Walkway, to break into four quadrants. Participants quickly navigated clockwise and then counterclockwise to each quadrant, making contact with both feet and facing forward. The PKMAS software provided 6 data points that gave insight on sequencing skills and balance reflective of mobility in daily life, including duration to complete and changes in main support.

Subjective Measures
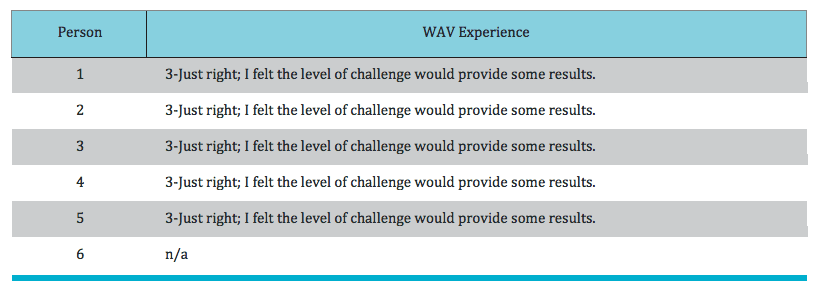
Following post exercise objective testing, participants were asked to complete a short questionnaire about their experience. The questions and participant responses are included below.
Q1. Which statement best matches your WAV experience today? (1-Way too Challenging, I wouldn’t do this again., 2-It was a bit too challenging; I’d prefer simplifying the exercises., 3-Just Right; I felt the level of challenge would provide some results., 4-It wasn’t quite challenging enough; I’d prefer more progressed exercises., 5-Way too easy; I don’t think I’d get any benefit.]