
by Polly Swingle, PT, GCS, CEEAA
An estimated 116 million Americans experience chronic pain each year. The national cost is $560 to $635 billion annually for medical treatment, lost work, and lost wages.
The causes of chronic pain vary widely. While many conditions can lead to chronic pain, certain medical conditions are more likely to cause it. These include: trauma/injury, diabetes, fibromyalgia, limb amputation, and reflex sympathetic dystrophy. Chronic pain affects each person differently and in some cases can lead to decreased activity, job loss, financial difficulties, anxiety, depression, and disability. With effective treatment, however, the negative effects of chronic pain can be reduced.
Pain Management Across the Spectrum
Headquartered in Livonia, Mich, The Recovery Project leverages cutting-edge, evidence-based research to provide progressive and effective physical, occupational, and speech therapies to clients who have suffered spinal cord, neurological, and traumatic brain injuries.
The Recovery Project strives to create hope and life-changing results for clients and their support networks across Southeast Michigan. The Recovery Project’s mission is to provide all of its patients the highest possible quality of life. The practice embraces frequent moderate-to-high-intensity therapy and cutting-edge rehabilitative science, and its therapists specialize in working with highly motivated individuals who are determined to let their recovery, not their injury, define their life. Education and learning remain at the heart of the organization’s professional identity.
Planning a Pain Management Program for a Diverse Clientele
The practice treats a diverse group of patients experiencing chronic pain. Those patients include individuals who have suffered spinal cord injuries and subsequent neurological impairment. Because such injuries can and do affect peripheral nerves, the associated pain can be chronic and potentially disabling, significantly impacting the quality of life for some patients. Some of the practice’s patients have had a traumatic brain injury (TBI)—a population that also experiences various forms and degrees of paralysis. TBI patients often struggle with involuntary joint contracture, which can lead to challenging chronic pain issues.
Some of the practice’s chronic pain patients are recovering from a stroke and are dealing with a condition formerly known as Reflex Sympathetic Dystrophy (RSD), now more properly referred to as Complex Regional Pain Syndrome (CRPS). The associated pain from CRPS, a disorder of the parasympathetic nervous system that can lead to redness, inflammation, and hypersensitivity to touch in the extremities, can be excruciating. Amputees dealing with chronic pain difficulties are part of the patient population: phantom limb pain in a distal extremity can be anywhere from distracting to debilitating.
The Recovery Project adheres to the National Institute of Health (NIH) position that chronic pain treatment needs to evolve from a one-pill-fits-all mind-set to an evidence-based, individualized, multidisciplinary model that recognizes the values of physical therapy and nonpharmacological approaches. Together, the prevalence of chronic pain and the increase of opioids have created a toxic combination of distress, disability, and danger to a large percentage of chronic pain patients. Chronic pain sufferers have typically been lumped into a single category, and treatment approaches have been generalized with little evidence to support this practice. Physical therapy is a non-pharmacological treatment that has proven to be highly effective. The problem is the lack of knowledge or limited availability of these nonpharmacological modalities, as well as the ready availability of pharmacological options and an associated reimbursements structure that steers clinicians to the use of opioids.
Technologies and Modalities
The practice utilizes a range of technologies, tactics, and techniques to deliver evidence-guided treatments that help its clients deal with chronic pain. While the specific set of tools varies, the basic treatment principles used include the following:
Education
Improving knowledge and understanding of chronic pain—how it occurs, and what can be done about it—including how brain and central nervous system hypersensitivity contribute to chronic pain. Therapists work closely with patients, teaching them how to manage pain and work toward performing the normal activities of daily living.
Strengthening and flexibility exercises
A therapist will design a program of graded exercises according to your abilities. Graded exercises help improve coordination and movement, reduce the stress and strain on the body, and decrease pain. Carefully introducing a graded exercise program will help train your brain to sense where the problems are in your body without increasing its danger messages.
Manual therapy
Specific, gentle, hands-on techniques that may be used to manipulate or mobilize tight joints structures and soft tissues. Manual therapy is used to increase range of motion, improve tissue quality, and reduce pain.
Postural Awareness and body Mechanics Instruction
This training helps improve posture and movement, allowing patients to use their bodies more efficiently while performing chores or recreational activities, reducing pain and increasing functional ability (including sleeping).
The specific tools and technologies used to treat chronic pain patients depend on individual condition and symptoms. For example, CRPS patients typically benefit from manual therapy and range-of-motion assistance, while amputees may be treated with a combination of mirror therapy, weight-bearing exercises, and the application of electrical stimulation. Specialized equipment that delivers forms of electrical stimulation can effectively mask the original pain sensation and “trick” the brain into no longer feeling the chronic pain.
Some chronic pain sufferers may derive short-term benefit from ultrasound therapy, but peer-reviewed evidence suggests that ultrasound treatments are beneficial/effective for approximately 12 treatments, and have limited efficacy thereafter. Consequently, they are not typically featured for chronic pain.
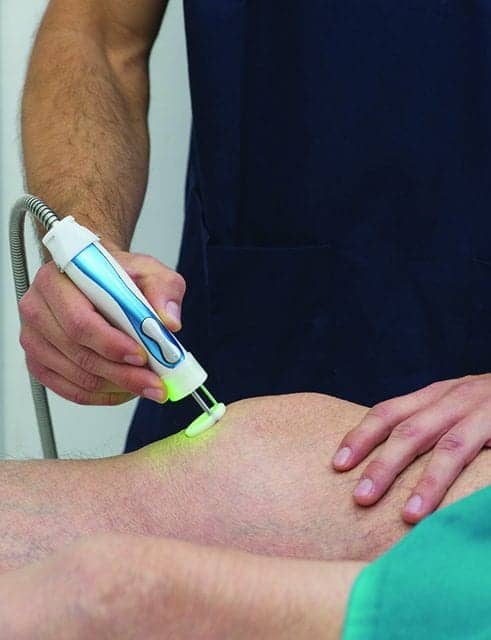
Peer-reviewed evidence shows that class 3B and IV lasers are also beneficial in the treatment of chronic pain. The effect is photochemical, not thermal. Lasers trigger a biochemical change on the cellular level that allows:
• The site of injury to promote healing, remodeling, and reduce inflammation;
• Lymph nodes to reduce edema and inflammation;
• Nerves to induce analgesia; and
• Trigger points to reduce tenderness and relax contracted muscle fibers.
Treatment times per point are in the range of 30 to 60 seconds. As few as one point may be treated in simple cases, but as many as 10 to 15 points may be treated for more complex dysfunction, such as cervical or lumbar radiculopathy.
Despite their use by some therapeutic service providers, the use of topical ointments, as well as ice, heat, or electrical stimulation, has not been found to be helpful in treatment approaches for chronic pain.
Goal Setting and Outcomes
As described earlier in this article, patient education is an important pillar of the practice’s therapeutic approach for treating chronic pain. Patient education—which is not just about exercise, alignment and posture, but also about nutrition, sleep hygiene, and general health and wellness tips and best practices—helps empower and motivate chronic pain patients. Most importantly, it helps them with day-to-day life tasks and teaches them how to move and function more efficiently in ways that minimize unnecessary movement, stress and pain.
When it comes to setting therapeutic goals, the general approach is to start small and build. Evidence demonstrates that patients must buy into the plan for maximum efficacy, so all decisions about goals are made collaboratively with the patient involved. Those decisions are made with the guidance of a full therapeutic team. Evidence shows that a multi-disciplinary management program that consists of a team of doctors and other healthcare professionals achieves better results. At The Recovery Project, that team typically includes a physician, a physical/occupational therapist, and a psychologist—one who is equipped to help with anxiety or depression and assist with cognitive behavioral therapy.
Conclusions
Because every chronic pain patient we treat has a secondary neurological diagnosis, the equipment we use is designed to achieve multiple goals: assisting with neuroplasticity recovery—gaining strength throughout the peripheral nervous system—but also getting people moving. Even patients with missing or compromised extremities can realize significant pain-management benefits from increased activity.
Suspension-sling systems that allow for gravity-eliminated exercise take weight off a patient’s musculoskeletal system. And less strain on the joints can help with improved range of motion and better outcomes. Weight-supported treadmills and other equipment that helps with postural awareness and body mechanics can be cross-leveraged from other therapeutic applications to treat chronic pain patients. Those therapies, when performed under the professional supervision of a physical therapist specifically trained to treat chronic pain, can be life-changing. RM
Polly Swingle, PT, GCS, CEEAA, is co-founder and lead physical therapist of The Recovery Project, which provides progressive, effective, evidence-based neuro rehab therapies aimed to improve quality of life and function of patients with spinal cord, neurological, and traumatic brain injuries at its three Michigan-based locations. For more information, contact [email protected].

My heart goes out to the families all over whom have been affected. In the last 5years I’ve had at least 6 surgeries and I still deal with pain from day to day. The surgeries have been with bones in different places on my body. I’ve not one time had a set back of being addicted to medication and everyone pain is not the same.
As a chronic pain sufferer I know first hand how disabling pain can be. Getting the body to move does helo but there are times that sufferers do need pain meds. I understand the taboo of these opoids but must sufferers are not addicted . There may be psychological needs for the meds but not in aw way like abusers. This programs sounds great but It may be a little unfair and unhealthy to think someone in severe pain like RSD to be able to function without opiods. It is easy to think medications are not helpful when your not a chronic sufferer. The need to treat without medications are easy to think for a non sufferer. Real pain sufferers are the ones being hurt by the rush need nit to prescribe and physical therapy alone.