|
| Cynthia Bauer, PT, DPT, OCS, is director of musculoskeletal outpatient services at Good Shepherd Rehabilitation Network, Allentown, Pa. |
Although most workers take their healthy shoulders for granted, imagine a graphic designer unable to move a mouse, or a delivery person incapable of lifting a box, or a fireman straining to pull on an oxygen tank. Such common workday tasks would be difficult without a fully functioning shoulder. The shoulder is a unique joint that can move in multiple planes with both strength and remarkable agility. When shoulders are injured on the job due to repetitive use or a sudden pull or strain, PTs use a wide range of therapies, pain-reducing modalities, and strengthening exercises to heal the shoulder and help workers—and their shoulders—return to on their jobs.
LIFTING, PULLING, PUSHING…
When the policeman is directing traffic or the toolmaker is crafting steel with a heavy machine tool, the shoulder is working, simultaneously conducting a symphony of muscles, ligaments, tendons, and bones to accomplish the required tasks at hand.
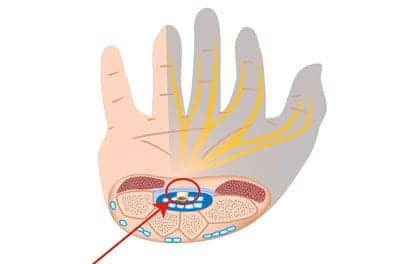
Three joints make up the shoulder, including the acromioclavicular joint, which joins the clavicle and the scapula, and the sternoclavicular joint, which attaches the clavicle to the top of the sternum. However, the third joint, technically known as the glenohumeral joint, is the main workhorse of the shoulder and is commonly referred to as “the shoulder joint.” The glenohumeral joint is a ball-and-socket-type joint that allows the arm to rotate in a circular motion to direct traffic, or to pivot out, up, and away from the body—useful for placing a crate of bananas onto a truck or helping a person into a wheelchair.
Various muscles, tendons, and ligaments support the three shoulder joints and their multidirectional functions. The rotator cuff, which is commonly torn by trauma or wear, gives the shoulder much of its agility and strength. It is comprised of several tendons and muscles that help connect the ball of the humerus to the glenoid socket.
When an injury strikes any part of the shoulder’s intricate structure, pain sets in and work slows down or stops altogether.
The common causes of shoulder injuries at work are due to overuse and repetition. Factory workers and other laborers are often susceptible, as they perform routine, repetitive tasks such as overhead lifting and pulling on heavy objects for 7 to 8 hours per day, 5 days per week, with little rest to allow the muscles and tendons to recuperate. Just as common are shoulder injuries from falls, in which the person’s arm reaches out to break the fall. If the force is overwhelming, it may tear muscles or dislocate the shoulder, pulling the ball out of its socket.
The most prevalent shoulder conditions are rotator cuff tears, rotator cuff tendonitis, impingement of the rotator cuff, bicipital tendonitis, and frozen shoulder.
Cynthia Bauer, PT, DPT, OCS, and director of musculoskeletal outpatient services for Good Shepherd Rehabilitation Network, Allentown, Pa, sees many overuse injuries from repetitive movements. “The muscles of the shoulder work synchronously,” Bauer explains. “Occasionally, some muscles can be stronger than the opposing or supporting group of muscles. Therefore, the motion may not be exactly smooth or congruent, causing the bones to compress or pinch tissues around the shoulder complex. This leads to a common shoulder condition called ‘impingement syndrome.’ When an individual works in a position that requires frequent shoulder reaching into the impingement position, inflammation and pain can occur.”
 |
| Cynthia Bauer, PT, DPT, OCS (right), applies electrical stimulation therapy on patient Jennifer M. West. |
Ironically, the underuse of a damaged shoulder joint can cause frozen shoulder, or “adhesive capsulitis,” which occurs in the joint’s capsule. The shoulder’s capsule is a soft-tissue covering that surrounds the glenohumeral joint and is attached to the scapula, humerus, and top of the bicep muscle. When a worker protects an injured arm through immobilization (for example, by placing the arm in a sling), the shoulder capsule’s tissues can form folds that stick together, thereby causing excessive tightness in the joint.
OVERALL SHOULDER THERAPY
These days, it is not uncommon for shoulder-surgery patients to have their first physical therapy appointment the next day after the surgery. Aside from following the surgeon’s recommendations, PTs treat each patient individually, initially evaluating the patient’s range of motion (ROM), strength, dexterity, reflexes, and pain before beginning therapy.
Depending on the condition and patient, PTs maintain a basic strategy and implement various therapies available to them. For rotator cuff surgical repairs, Bauer says her protocol is to first follow the surgeon’s recommendations and to protect the surgical site. “We begin with gentle passive range of motion. The surgeon has just sutured tissues, and they need to heal. Patients are apprehensive about pain, and this is not the time to push aggressively or cause pain.” She says, “Then, little by little, we begin increasing the stretching and start with gentle exercises, progressing to strengthening as part of their program. Our therapists use manual stretching; mobilization of the shoulder; and add modalities to relieve pain, relax muscles, or reduce inflammation. Some modalities include heat, electric stimulation, ice, ultrasound, and others. Then, gradually over time, the exercises become more difficult and continue until the patient returns to their maximal function and strength.”
Bauer adds that, especially for injured workers, shoulder muscles must maintain a level of endurance. She says, “It is important to determine what activities a worker does during the workday. Many jobs require endurance of the shoulder muscles. If that is a requirement at their job, we address improving endurance with the exercises that we choose. We also give them a home program to support what we’re doing at the clinic.”
Proper posture is also important, because poor posture can lead to asymmetrical development or strength in certain muscles so that the muscles are not working synchronously. “Some of the muscles that work around the shoulder are small, stabilizing muscles,” Bauer says. “They’re not the big, forceful muscles. When you picture a muscular body, you may think of big pectoral muscles, large deltoids (shoulders), and big back muscles, but you don’t see these little rotator cuff muscles that are supporting the shoulder and contributing to the normal strength and function. We need to get these little muscles working appropriately with the bigger muscles so they do not overpower them. So we prescribe shoulder-stabilization exercises to enhance stability of the shoulder.”
 |
| Cynthia Bauer, PT, DPT, OCS (left), oversees Larry Fehr’s therapy on a CPM unit. |
REHAB TECHNIQUES TO EMPLOY
PTs and OTs have a wide range of therapy techniques that can be implemented for shoulder rehabilitation. As soon as 1 day after a shoulder surgery, a therapist can begin rehab through passive ROM exercises, where the therapist will gently manipulate the shoulder through the patient’s tolerable ROM.
Exercises for postop shoulder patients generally follow the progression of passive ROM and/or active ROM, and light passive resistance for all planes of the shoulder, which may include flexion extension, abduction, adduction internal and external rotation.
A rotator cuff repair patient generally will not start active range of motion or passive resistance exercises until approximately 4 to 6 weeks after surgery. Instead, exercises would focus more on functional and closed-chain type exercises.
Very shortly after shoulder surgery, a physician may recommend continuous passive motion (CPM) therapy. Some CPM machines can be used in a hospital bed, while others can be used as stand-alone machines in the machine’s built-in chair. Various types of CPM machines have the ability to mechanically, yet gently, move the joint through its natural range of motion safely while maintaining minimal scapular movement. CPM machines do not replace the benefits of active, hands-on therapy, but they do have the ability to precisely control the ROM and force applied to the joint, as well as detect resistance on the part of the patients. Among CPM’s benefits are the alleviation of stiffness and pain, a decrease in the potential for developing scar tissue, and an increase the ROM, all of which may lead to shorter rehabilitation and faster recovery time.
TOOLS OF THE TRADE
Bauer says, “A good therapist is going to accommodate their strengthening program and techniques to meet the needs of the client, and that’s one of the most important things with therapy. It’s the manual aspect. The therapist guides the patient in strengthening their shoulder using manual techniques or the ‘hand-on’ approach. We also use equipment that we have available.” There is a huge selection of therapy equipment designed for shoulders and occupational therapy. The equipment that a therapist chooses will depend on the rehabilitation center, but may include upper-body ergometers, plyoballs, medicine balls, dumbbells, strengthening machines, exercise bands, shoulder-stabilization equipment, isokinetic machines, as well as work-specific strengthening equipment.
Exercise balls, weighted and of various sizes, can build strength, endurance, and ROM with exercises that mimic work situations, such as lifting and handling packages and placing items over the head. Holding a ball with two hands, patients can extend their arms over their head, side to side, or toss the ball to a partner or against the wall, increasing strength, ROM, and agility.
Flexible bands help exercise and strengthen the shoulder through resistive movements that provide both positive and negative force on the muscles, improving strength, and cooperation of muscle groups. Exercise bands are inexpensive, portable, and often color-coded, with each color representing a different level of resistance.
Other equipment that therapists may use for shoulder rehab may include: a trampoline used with a weighted 2- to 6-pound ball, which a client will throw against the trampoline and catch, helping with the shoulder’s strength and reflexes; an arm bicycle that can be used for warm-up exercises and for increasing the patient’s endurance; and, shoulder pulleys to help stretch shoulder joints and muscles in various planes via a variety of exercises (these are inexpensive and easy to set up on any door, and may be especially useful for stretching frozen shoulders for home therapy).
For those who wish to get back to Pilates, tai-chi, or yoga, most therapists do not recommend such exercises for any acute or short-term rehab, but they may be a part of long-term rehab program. Whatever exercises are used, good posture should be maintained without any sharp, forceful movements that may reinjure the joint.
BEFORE RETURNING TO WORK
After they complete the acute physical therapy on their shoulder injuries, many workers continue more specific job-related rehab therapy with occupational therapists, who will simulate the tasks workers perform on a daily basis.
For example, an OT can simulate weight-lifting requirements, how often a person needs to lift in a day, whether the patient has to climb into or out of a truck or turn a wheel, among other tasks. OTs work on endurance and practicing the job, as well as teaching the patient how to prevent future injuries.
Occupational therapy programs can last 4 to 8 weeks, and sessions can last 3 to 5 days per week for 2 to 3 hours. By the end, the patient’s shoulder is reevaluated, and then, hopefully, the shoulder is ready to get back to work full-time.
Tor Valenza is a staff writer for Rehab Management. He can be reached at .